


JOHN LI, M.D.
OTOLOGY NEUROTOLOGY RESOURCES
210 Jupiter Lakes Blvd #5105
Jupiter, FL 33458
Phone: (561)-748-4445
Fax: (561)-748-4449
Transtympanic Medication
Early concept of a transtympanic perfusion device developed in the 90's
Applications Imagine the possibilities of removing toxins directly from the inner ear to prevent or even reverse deafness. Imagine being able to focus high concentrations of certain medicines that would otherwise too powerful to give intravenously. Imagine being able to stop vertigo. The list goes on and on. In 1998, Dr. Li and Dr. Gianoli ran one of the earliest studies on the use of Transtympanic Steroids on Sudden Hearing Loss to evaluate it's effects. See the summary here.
Sudden hearing loss Sometimes, people lose hearing the suddenly without any apparent reason. The treatment for this sudden onset hearing loss is typically oral or intravenous steroids. However, sometimes patients cannot tolerate the doses required by oral or intravenous administration. In these cases, direct application to the inner ear through the transtympanic route may be the only option. Transtympanic Steroid perfusion has been used in the treatment of sudden onset sensorineural hearing loss and Meniere's disease. It may have applications in hearing protection and regeneration. Steroids calm inflamed balance organs and nerves. If taken by mouth or intravenously, steroids have many potentially bad side effects. These side effects are greatly reduced because the medicine is directly placed into the ear.
Meniere's Disease and Intractable Persistent Vertigo Sometimes, one inner ear can become so damaged and so problematic that it causes terrible vertigo. If it cannot be rehabilitated or fixed, it may need to be shut down. (an intermittently flashing light is more annoying than one that is turned off) In the past, one would have to resort to a neurosurgical (brain surgery) approach to cut the balance nerve to prevent further attacks of vertigo. Now we simply need to make a small pin hole in the eardrum and infuse medicine directly into the affected ear. (If you gave the medications intravenously or intramuscularly, both ears might be damaged.) Streptomycin or Gentamicin Perfusion: An outpatient procedure. An antibiotic that is toxic specifically to the balance nerve is placed through a small puncture in the eardrum. This antibiotic essentially kills the already damaged balance nerve and usually (85-95%) spares the hearing. Success has been reported to be about 80 -- 90% although relapses are possible. 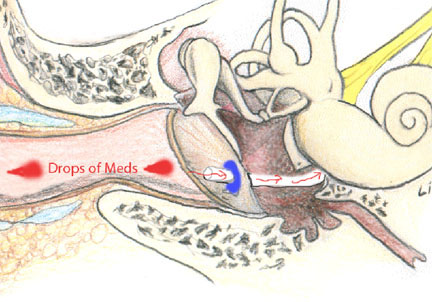
Transtympanic medications can be administered using one of several methods. The simplest method is through a tiny needle puncture of the eardrum. This can be done easily in the office with or without a little bit of numbing medicine. If multiple injections are required, a small ear tube (myringotomy tube) can be done in the office with a little bit of numbing medicine. Another development has been the Silverstein microwick, which utilizes a sponge like wick inserted through a tiny ear tube to guide the medication to the round window of the inner ear. That way, one can simply place the medication as drops in the ear, and it will be absorbed. Our usual protocol is to place an ear tube under local anesthesia in the office. For sudden hearing loss, we schedule 5 or 6 injections of Steroids (Dexamethasone) every other day over a 2 week span. For Meniere's Disease, we do something similar, but may stop earlier after 1, 2 or 3 injections. Patients come to the office for these procedures. For those who are travelling from far away or who want general twilight anesthesia, we sometime use the Silverstein microwick. Patients can apply the medications themselves since the wick replaces a need for the needle, and can avoid the every other day drive to the office.
Patient information "The idea behind transtympanic medication is that we can concentrate the dose of medication and deliver it to the target ear by delivering it directly to the target. Oral medications and intravenous medications need to be distributed throughout the whole body before it gets to the target. Oftentimes, the drug is degraded (metabolized) and thus less effective by the time it gets to the intended site. Transtympanic medication should have less systemic (bodily) side effects, and smaller amounts of drug can be used." "This minor procedure can be done in the office with local anesthesia. There is usually little in the way of pain. It usually takes about 15 or 20 minutes to perform." "The downside of transtympanic medication is that it requires that a minor procedure be performed. A small incision needs to be made in the ear drum to get the medication to the target organ."
Complications: The risks and complications of the surgery are the same as for the insertion of tympanostomy (myringotomy) tubes. In general, they are very minimal and rare. As with any surgery; pain, bleeding, infection and drainage can occur. If a tube is placed, it usually falls out on its own within a few weeks or months. Usually the hole will close on its own. In rare instances (< 3 percent), the hole persists and will require closure at a later date. Temporary dizziness is quite possible. On the other hand, long-term dizziness, ringing in the ears, and hearing loss are quite rare. Typically, as with any office procedure, I recommend that the patient does not drive or operate heavy machinery for at least six hours (or more) afterwards. The standard treatment for sudden onset sensorineural hearing loss is oral steroids. "Steroids are used to treat sudden onset sensorineural hearing loss because they are potent anti-inflammatory medications. When the cells of the inner ear suddenly stop working, giving steroids is like doing CPR. The idea is to resuscitate the hearing hair cells before they die. The time window for doing this can be up to six months. However, the sooner the steroids are given, the better. We prefer to get it done before two weeks have elapsed." "Sudden hearing loss that occurred more than six months ago is not likely to respond to transtympanic steroids (or oral steroids for that matter.)"
|