


JOHN LI, M.D.
OTOLOGY NEUROTOLOGY RESOURCES
210 Jupiter Lakes Blvd #5105
Jupiter, FL 33458
Phone: (561)-748-4445
Fax: (561)-748-4449
BPPV Canalith Repositioning The 360 Maneuver & Repositioning Chair Surgery for BPPV Posterior Canal Occlusion
The Canalith Repositioning Procedure (CRP / Epley Maneuver)
The following is part of our online manual. Note that our form of CRP is very different from the Semont maneuver which we find too forceful for practical use.
How is it done?
In Optimized CRP, pre-medication to prevent nausea or vomiting is usually not necessary except in severely affected anxious patients. The patient begins the procedure in a sitting position. The head is turned toward the affected side. A mastoid bone oscillator is applied and held in position to the mastoid of the affected ear by a head band. This frees up the operator to help with patient positioning. The headband is applied such that the Velcro straps are over the occiput. The oscillator is then slipped under the band on the affected side.
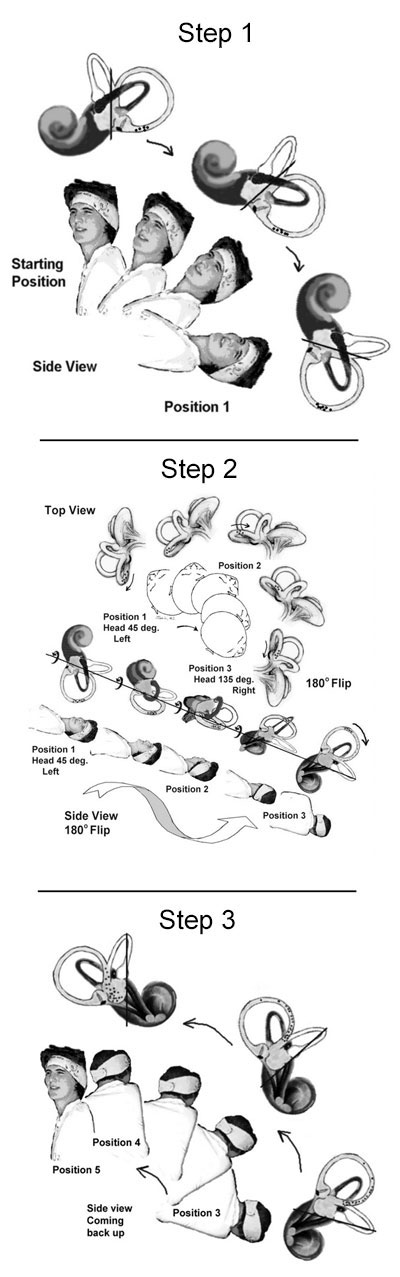
The patient is then slowly reclined to the Dix-Hallpike position of the affected side. The rate is titrated to the point of no nystagmus and no symptoms. This usually takes about 40 seconds. Another 20 seconds are spent in that Dix-Hallpike position (affected ear down).
Next, the patient's head is slowly turned to the opposite side and the body rolled such that the shoulders are aligned perpendicularly to the floor (affected ear up). The head is then turned further so that the nose points 30 degrees below the plane of the chair. This usually takes another 40 seconds.
If no nystagmus is seen, the patient is then raised back to the sitting position. Finally, the head is turned back to the midline. These positions are demonstrated in Fig. 1. A Dix-Hallpike test is done immediately following the procedure. If nystagmus is seen, the procedure is repeated. After the procedure the patient is instructed to avoid agitation of the head for about 48 hours while the particles settle. They are also asked to return in one week for follow-up exam.
Pointers:
The specially designed headband holds a model of the posterior semicircular canal containing simulated canaliths. The model is spatially oriented to approximate the position of the actual (ipsilateral) posterior semicircular canal. By watching the particles flowing within the model, a novice operator (or even the patient) can have instant feedback as to the effect each repositioning maneuver has on the canalithiasis. If done correctly, the particles should flow in the direction marked by the arrows on the headband from the start position (representing the nerve filled ampulla of the posterior semicircular canal) to the end position (representing the vestibule in which the particles cannot irritate any nerve structures). Care should be taken to prevent reflux (movement opposite to arrows) of particles back to the ampulla.
Rather than going suddenly from position to position , an emphasis is made on moving the patient gradually, at a pace that does not generate any rotatory nystagmus. If nystagmus is induced, motion is suspended until the nystagmus goes away. The gradual (rather than sudden) change in head position prevents "fluid lock". A simple example of fluid lock can be demonstrated in a ketchup or salad dressing bottle. The viscous fluid flows better when gradually tilted to an angle than when suddenly inverted. When the fluid does flow after sudden inversion, it occurs somewhat more violently. In the inner ear, this turbulent movement of canaliths seems to cause the dizziness. Slow deliberate movements avoids this dizziness and is preferred by patients. Constant mastoid vibration seems to help the canaliths move within the semicircular canals much like shaking the ketchup bottle helps the flow of ketchup.
Related Pages
BPPV Canalith Repositioning The 360 Maneuver & Repositioning Chair Surgery for BPPV Posterior Canal Occlusion
External Articles, authored by Dr. Li in E-Medicine Online and Medscape
Medscape: BPPV Medscape: BPPV Clinical Presentation ENT Today: BPPV Diagnosis and Treatment