


JOHN LI, M.D.
OTOLOGY NEUROTOLOGY RESOURCES
210 Jupiter Lakes Blvd #5105
Jupiter, FL 33458
Phone: (561)-748-4445
Fax: (561)-748-4449
BPPV Canalith Repositioning The 360 Maneuver & Repositioning Chair Surgery for BPPV Posterior Canal Occlusion
The Multiaxial Chair for the "360 Maneuver"
"The Multiaxial chair was developed to allow for a pure 360 rotation of the semicircular canals. It uses the same concept of the Epley Maneuver. In fact, it can sometimes work when the standard repositioning procedures fail. We have physicians refer these difficult patients from all over the world."
"The Multiaxial chair was developed to allow for a pure 360 rotation of the semicircular canals. It uses the same concept of the Epley Maneuver. In fact, it can sometimes work when the standard repositioning procedures fail. We have physicians refer these difficult patients from all over the world."
Introduction

As canalith repositioning becomes more accepted in the treatment of benign positional vertigo, straightforward cases are more readily recognized, treated and cured using standard repositioning maneuvers by the general medical community. Difficult cases and those that fail standard treatment are the ones that are referred. Thus referral centers are seeing a skewed population of more difficult BPPV cases. It seems that in some of these cases, the standard Epley maneuvers either cannot be physically done or fail to solve the problem. These difficult cases require a different approach. A multiaxial positioning device has been developed to treat the more difficult patients.
Advantages
Difficult patients are represented by those who are unable to physically tolerate body position manipulation, patients who are prone to panic, patients who have canal particles in more than one canal, and patients in whom standard repositioning maneuvers are ineffective.
Some patients have back problems that are exacerbated by flexion, extension or torsion, and are therefore unable to physically tolerate the body position manipulation. Both the Epley and Semont maneuvers inherently require some degree of torsion, extension and flexion. Patients who have had strokes or some sort of paralysis also have a difficult time facilitating the maneuver. The multiaxial positioning device allows the patient to be secured in a chair and immobilized. All positioning is done externally with the body as a unit. There are no elements of flexion, extension or torsion involved. The patient does not have to move a muscle.
Patients who are prone to panic attacks are also difficult to reposition. Some will not allow themselves to be placed in a Dix Hallpike position. Those who allow the practitioner to start the maneuver often find themselves fighting violently and uncontrollably to recover to the upright position. The multiaxial positioning device allows the patient to be strapped securely to the seat. There is security in knowing that they cannot fall. Since they are physically restrained, they cannot flail about. This allows the procedure to be done while preventing the patient from physically harming himself and others.
Patients who fail the standard repositioning maneuvers may simply require a pure 360 degree rotation. The multiaxial positioning device may actually help distinguish certain conditions such as canal jam, cupulolithiasis or involvement of multiple canals. (9,10,11)
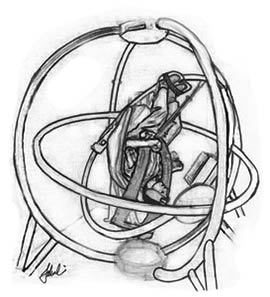
The Device
The multi-axial position device consists of two concentric rings in a stabilizing frame. In the center ring, a bucket seat with padded metal shoulder and torso harness (similar to that used in modern-day roller coaster rides) is used to secure the patient snugly in the seat. Two DC motors were mounted to drive the rotation about the vertical and horizontal axes. In order to get electrical current to the inner ring, two slip rings were incorporated into the two axes. This Device was actually built from an amusement park ride, adapted to suit the needs of the360 maneuvers.
 | 
|
Concept to reality
Results and Conclusions
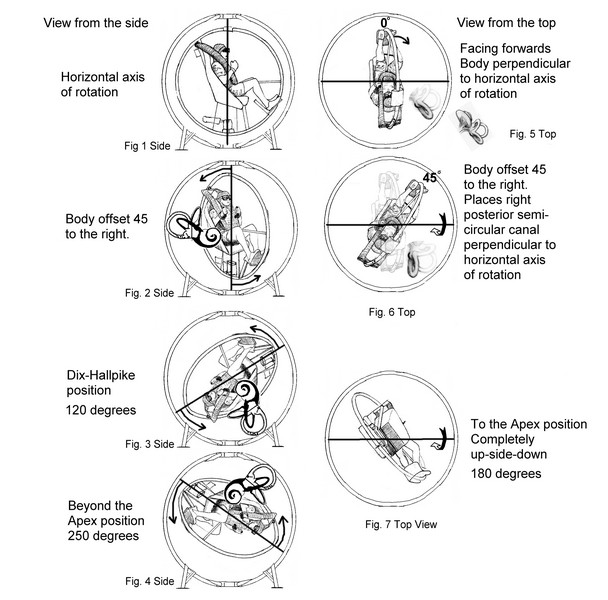
The 360 degree maneuver can be effective in treating benign positional vertigo. Its rate of success is comparable if not superior to the rate of success of the standard Epley maneuver. This success is not surprising given that careful analysis shows that the positions of the Epley maneuver as well as the Semont maneuver correlate with positions reached using the 360 maneuver and thus are quite similar. The procedure itself is generally not uncomfortable and fairly well tolerated by patients. Validation of the 360 maneuver opens the doors for further research in the treatment of difficult vertigo patients. We have found that patients who have failed standard repositioning can sometimes find success here.
Related Pages
BPPV Canalith Repositioning The 360 Maneuver & Repositioning Chair Surgery for BPPV Posterior Canal Occlusion
External Articles, authored by Dr. Li in E-Medicine Online and Medscape
Medscape: BPPV Medscape: BPPV Clinical Presentation ENT Today: BPPV Diagnosis and Treatment